


Meniscus injuries are among the most common knee injuries treated by orthopedic surgeons worldwide. They frequently occur in athletes, active individuals, and aging populations affected by degenerative changes.
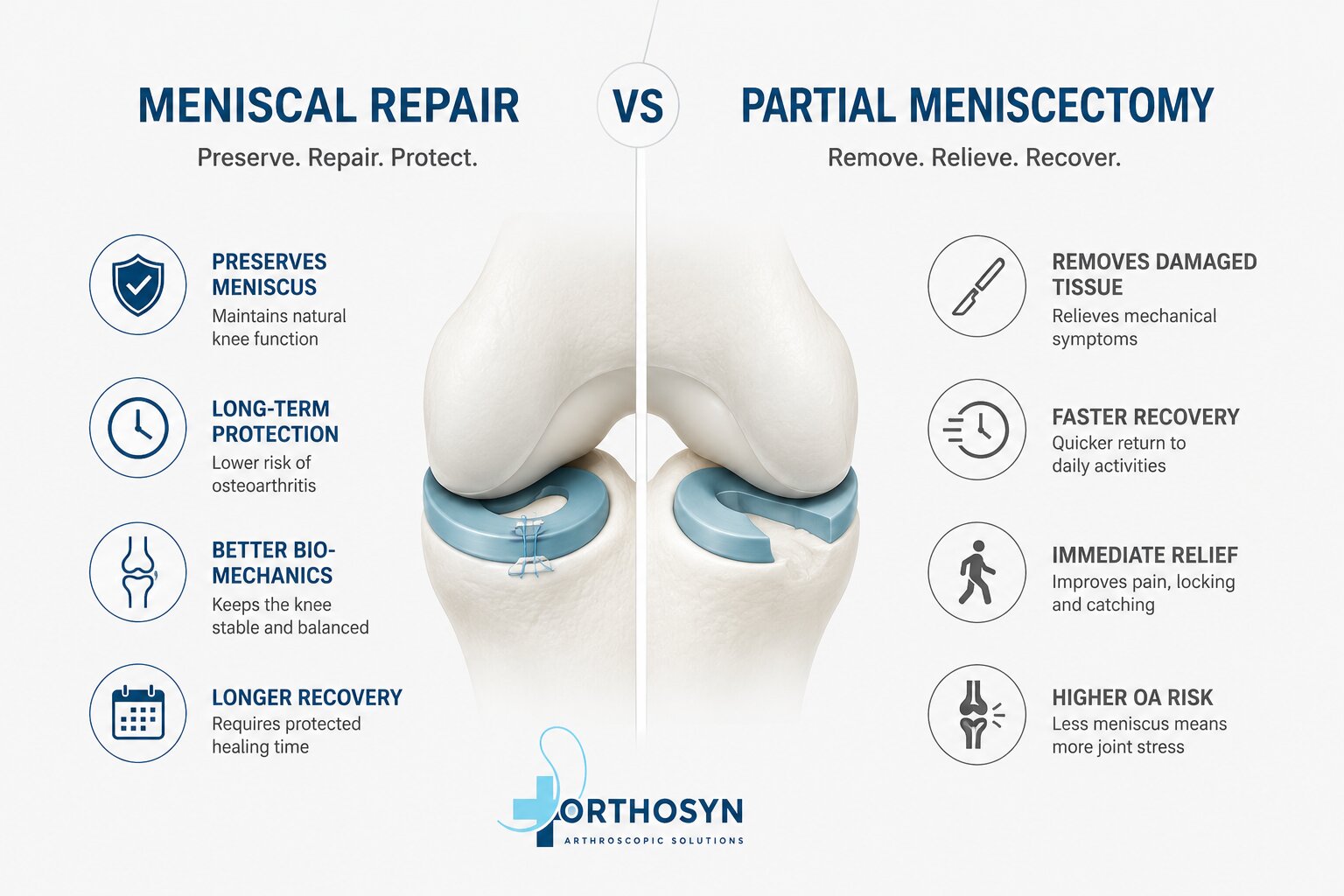
When conservative treatment fails, surgery may become necessary. The two most common surgical options are meniscal repair and partial meniscectomy.
Although both procedures aim to relieve symptoms and restore knee function, they have very different objectives and long-term implications.
Understanding the differences between these treatments helps physicians and patients make informed decisions regarding meniscus preservation and knee health.
The knee contains two menisci:
These fibrocartilaginous structures perform several critical functions:
Because the meniscus plays an important biomechanical role, preserving as much tissue as possible has become a major goal of modern orthopedic surgery.
Meniscal repair is a procedure designed to preserve the meniscus by suturing the torn tissue and allowing biological healing.
Instead of removing damaged tissue, the surgeon reattaches the torn segment and stabilizes it using specialized meniscal repair devices.
Modern arthroscopic techniques have significantly improved repair success rates.
The repaired meniscus continues to contribute to:
This helps maintain normal knee biomechanics.
Numerous studies have shown that preserving meniscal tissue may reduce the long-term risk of osteoarthritis.
Although recovery may take longer, successful repairs often provide superior long-term joint preservation.
Not every meniscal tear is repairable.
Factors affecting repairability include:
Healing also requires adequate blood supply.
Partial meniscectomy involves removing the damaged portion of the meniscus while preserving as much healthy tissue as possible.
This procedure is one of the most commonly performed arthroscopic knee surgeries.
Patients often return to daily activities more quickly than after meniscal repair.
Mechanical symptoms such as:
often improve rapidly.
The surgery is generally less complex than meniscal repair.
Removing meniscal tissue reduces its protective function.
Potential long-term consequences include:
For this reason, tissue preservation is increasingly prioritized whenever possible.
Meniscal repair is commonly considered for:
Especially vertical tears located in vascular regions.
Many bucket handle tears can be successfully repaired.
Particularly in younger patients.
Healing rates may improve when repair is performed alongside ACL reconstruction.
Partial meniscectomy may be considered when tears are:
The decision depends on intraoperative assessment.
Advances in arthroscopic technology have expanded repair possibilities.
Current options include:
The most commonly used modern technique.
Advantages include:
Traditionally considered the gold standard for certain tear patterns.
Often used for selected anterior horn lesions.
Modern meniscal repair systems allow surgeons to perform stable fixation while minimizing surgical trauma.
Benefits include:
Orthosyn Medikal offers arthroscopic meniscal repair solutions designed to support modern knee preservation procedures.
The Orthosyn Meniscal Repair System is developed for all-inside meniscus repair techniques and provides reliable fixation during arthroscopic procedures.
These solutions support surgeons seeking to preserve meniscal tissue whenever clinically appropriate.
| Factor | Meniscal Repair | Partial Meniscectomy |
|---|---|---|
| Tissue Preservation | Excellent | Limited |
| Recovery Speed | Slower | Faster |
| Osteoarthritis Risk | Lower | Higher |
| Technical Complexity | Higher | Lower |
| Long-Term Joint Protection | Better | Reduced |
| Healing Requirement | Necessary | Not Required |
Modern orthopedic surgery increasingly favors meniscal preservation whenever possible.
Meniscal repair offers important long-term benefits by maintaining knee biomechanics and potentially reducing future osteoarthritis risk.
Partial meniscectomy remains an effective solution for tears that cannot be repaired.
The optimal treatment depends on tear characteristics, patient factors, and surgical evaluation.